There are two reasons why investigating incident and accident should be done. The first reason is to determine their cause and the second is so that information forthcoming from the investigation can be used to prevent them happening again.
- Why accidents and incidents should be investigated
- Legal reasons for investigating accidents and incidents
- Financial reasons for investigating accidents and incidents
- Other reasons for investigating accidents and incidents
- Benefits from investigating accidents and incidents
- Near misses and dangerous occurrences
- Categorizing incidents
- Training for the investigating team
- The accident/incident investigation
- Analysing causes of an accident
- Accident/incident report forms
- The importance of learning lessons from major incidents, management, cultural and technical failures that may lead to such incidents
- Learning the lessons
- Learning lessons locally
- Learning lessons more widely
- Revision questions for element 1
Why accidents and incidents should be investigated
An investigation should not be used as a vehicle to apportion blame for an accident or incident. Employees should be encouraged to give their full co-operation to the investigating team, and this would perhaps be compromised if they thought that by doing so they might be held responsible in some way for the event. There are risks and hazards within all workplaces, and measures are put in place to either eliminate them or reduce them to a level which is acceptable in order to prevent accidents or incidents which may be dangerous and/or result in injury, ill health or property damage. The very fact that an accident or incident has occurred means that those risk control measures current at the time are likely to have been less effective than expected. Furthermore, accidents and incidents need to be investigated for both legal and financial reasons.
Legal reasons for investigating accidents and incidents
To demonstrate that the company is meeting its legal requirement to investigate accidents and incidents.
Persons who have been affected by an accident may consider taking legal action against the company as a result. Consequently, employers should make available information regarding the circumstances appertaining to the accident which result from any investigation.
If needs be, a company can demonstrate to the courts their commitment and positive attitude to health and safety by providing evidence of a thorough investigation of an accident which subsequently allowed them to take steps to put in place measures to prevent any future recurrence.
Financial reasons for investigating accidents and incidents
Information forthcoming from an accident investigation provided to an insurance company may well assist in the event of a claim.
Investigating dangerous incidents and rectifying the cause, such as an escape of flammable vapour, could prevent a recurrence with potential catastrophic results, thus averting the cost of repairs and replacement and lost revenue, as well as potentially saving lives and preventing injuries.
Other reasons for investigating accidents and incidents
The information and insights gained from the investigation of accidents and incidents are invaluable. The following are examples of the kinds of things to be expected when a thorough investigation is conducted:
- How and why an accident/incident happened;
- What working practices and procedures actually are – these may differ from what they should be (e.g. employees may take unacceptable risks to make their work easier or faster);
- How exposure to conditions (e.g. noise, cold, heat) or substances (e.g. chemicals, radiation, gases) may affect the health of employees;
- Weaknesses or faults in production systems whereby a certain scenario of events will expose these weaknesses or faults;
For example, opening a flow valve too quickly might cause pressure to build up beyond a safe working pressure in a pipeline, resulting in an escape of flammable product from a flange. Remedial action would focus on safe working procedures, possible pressure relief systems or the strengthening of flanges; - An investigation can highlight weaknesses in existing risk control measures and allow employers to review and supplement them in order to prevent accidents/incidents in the future. Lessons learned in one department of an organization can be used in other departments, thus benefitting the organization as a whole.
Benefits from investigating accidents and incidents
As well as information and insights being gained from investigating accidents and incidents, there are also tangible benefits to be had. The following are examples of such benefits:
- The outcomes of an investigation can result in the company putting measures in place to prevent
the recurrence of similar accidents or incidents in the future; - The company can avoid business losses if they take heed of the outcome of an investigation by preventing further accidents or incidents. For example, the escape of flammable product we cited earlier which, in this case, was caught before it escalated into a potentially catastrophic incident. The benefits of remedial action can be measured in the number of potential lives saved as well as the potential savings of the cost of repairs and replacement and lost revenue. Other costs saved might include the cost of legal action which might be taken against the company; increased insurance premiums; and loss of business due to a bad reputation, resulting in lost orders;
- The development of a health and safety culture within the company. Following an investigation, any measures which are put in place as a result of the findings will be more readily accepted by the workforce, especially if they were involved in the decision-making process;
- Managerial skills will be developed during any investigation and these can be used in other departments within the organization.
Near misses and dangerous occurrences
Not only is the investigation of accidents and incidents important, it is also useful to investigate near misses and dangerous occurrences which did not result in injury. Just because no-one has been injured on one occasion does not mean that if the event happened again the result would be the same.
Whether the incident is classed as an accident, a near miss or a dangerous occurrence, the investigation should carry the same degree of importance, and the findings will be as useful in any event in preventing a recurrence. Specific lessons should be noted to identify why control measures already in place failed to prevent the incident and what further measures should be introduced to rectify the situation. General lessons learned from one incident will also be useful throughout an organization to increase awareness about health and safety issues.
Let’s take a look at case study involving a dangerous occurrence.
Case Study
On a production platform, the process system was being started up and the start-up procedure was being followed. Suddenly, and without warning, a fire was detected around a pipe flange within an unmanned and confined section. The fire and gas detection system immediately detected the fire and emergency procedures were immediately activated. These included the Emergency Shutdown (ESD) system which isolates the affected section of the process so as to stop the fire being fed by further flammable product. The Emergency Shutdown (ESD) system also brings to an end the process system. The fire extinguisher system, which in this case uses an inert gas, was activated in that confined area to extinguish the fire.
The investigation that followed found a number of failings. These included the fact that the start-up procedure had not been followed precisely. One of the flow valves had been opened too quickly, allowing product to flow too quickly. This had two effects.
First, pressure in the pipeline built up to a level which came near to the maximum operating pressure for that pipeline. This was exacerbated by the fact that the flange connection bolts had not been checked during routine maintenance work and did not have the required torque tightness to hold the maximum pressure of the pipeline, resulting in the leak of flammable product.
Second, the increased flow of product also served to create a build-up of static charge in the pipeline. The electrical bonding of the pipeline was found to be insufficient and a spark was generated which ignited the leak from the flange, resulting in the fire.
Conclusions from the investigations were:
- personnel involved in process systems, and in particular, start-up and shutdown, should be given more regular training, including a wider understanding of the consequences of certain actions; and
- a review of the extent and frequency of the maintenance programme should be conducted, with a view to making it more effective.
Categorizing incidents
Accidents and incidents result in outcomes. If accidents/ incidents are categorized under their various outcomes, it is possible to give them the appropriate degree of attention and/or investigation. For example, an accident where someone was hurt by tripping over a discarded box would not warrant the same level of investigation as an escape of hydrocarbon gas.
Let’s first deal with the word outcome, to make it quite clear what we are talking about.
An outcome is the effect of an unplanned, uncontrolled event and can range from a mere escape of vapour which causes no ill effects and disperses into the atmosphere, to a major incident with structural damage and a number of injuries.
An outcome can result in one of the following:
- Injury;
- Minor injury;
- Significant injury;
- Major injury;
- Dangerous Occurrence or Damage Only;
- Near miss.
Let’s look at what each of these outcomes means.
Outcome – injury
Injury is physical damage or harm which is suffered by a person.
- Minor injury – an injury which does not involve time off work;
- Significant injury – a significant injury is one which is not ‘major’ but which results in the injured person being away from work OR being unable to carry out their full range of normal duties;
- Major injury – major injuries are those which can be regarded as a serious threat to a person’s health and/or well-being.
Outcome – Dangerous Occurrence or Damage Only
A Dangerous Occurrence or Damage Only is an event that happens which has not involved injury to anyone, but which could have done. The following list of examples is not meant to be exhaustive:
- A fire or explosion not resulting in injury;
- An escape of flammable or toxic gas, vapour or fluid;
- The collapse, overturning or failure of load-bearing parts of lifts and lifting equipment;
- Explosion, collapse or bursting of any closed vessel or associated pipework;
- Electrical short circuit or overload causing a discharge spark;
- Failure of industrial radiography or irradiation equipment to de-energize or return to its safe position after the intended exposure period.
Outcome – near miss
A near miss is any unplanned incident, accident or emergency which did not result in an injury. An example would be materials falling from scaffolding and almost hitting an employee underneath. A near miss must be reported to determine the cause in order for changes to be made to prevent it happening again.

Training for the investigating team
Any accident/incident investigation will involve a team of people with different skills depending on where they work. All will have had previous training in accident investigation. A typical team will include:
- Operations team leader;
- Field or platform safety officer if it’s an offshore installation;
- Safety representatives;
- Area authorities (responsible for the area where the incident took place);
- Senior onshore managers;
- Specialist inspectors;
- Tool pusher if it’s a drilling rig.
The investigating team will need to have information and training regarding:
- Their roles and responsibilities;
- How to identify which events need to be reported;
- How to complete documentation;
- Accident book regulations and requirements and how to use it as a source of historical information;
- Documents and forms relevant to the investigation – internal and external;
- The importance of reporting accidents/incidents/ dangerous occurrences/near misses for legal, investigative and monitoring reasons;
- The dissemination of information and to whom.
The accident/incident investigation
There is a generally accepted four-stage process to investigating accidents/incidents.
- Step one – gathering the information;
- Step two – analysing the information;
- Step three – identifying the required risk control measures;
- Step four – formulation of the action plan and its implementation.
Let’s look at each of these steps in more detail.
The accident/incident investigation step 1 – gathering the information
Some of the information required to conduct the investigation will be taken from the scene of the incident, which must be kept secure and undisturbed until the team is satisfied that they have all the facts they need. This could be when all photographs, sketches and measurements have been made.
If the incident is serious enough to involve the enforcing authorities and/or police, then the area must be secured until permission has been given by those authorities to open the site.
Should the area pose a risk to others, then the area must be made safe but photographs should be taken if possible before the site is disturbed.
The process of gathering the information should ensure that it:
- Explores all reasonable lines of enquiry;
- Is timely – should be done as soon as possible after the event;
- Is structured, setting out clearly what is known, what is not known and records the investigative process.
This is the stage to collect information about:
- Where it happened;
- When it happened;
- Who was involved;
- What was involved.
Relevant information will include sketches, measurements, instrument readings and records, logged information, photographs, check sheets, permits-to-work and details of the environmental conditions at the time if relevant. Opinions, experiences and observations as well as events which led up to the accident/incident should also be recorded.
Gathering the information – observational techniques
Observation is an integral part of an investigation, and managers and supervisors will need to be trained in observational techniques. The observation of working procedures will identify those practices which are regarded as unsafe and which need to be changed in order to make them safe.
Good observation skills should include:
- Knowledge of the workplace and procedures;
- Being open minded;
- Keeping a systematic record of observations.
Each of these skills can help to ensure observations are done effectively.
Good observation relies on a number of additional techniques. The observer should:
- Take time to observe the whole scene;
- Be alert to possible changes to the accident scene by those who may have a motive to correct unsafe practices;
- Use the ABBI technique: look Above, Below, Behind, and Inside;
- Be inquisitive and question employees to determine risks – their views can be a valuable source of insight;
- Use all senses including smell, sight, touch and hearing;
- Have an open mind and look for solutions;
- Identify, record and feedback good performance as well as bad.
Gathering the information – interview techniques should include:
- Using an interviewing style which does not reflect a blame culture;
- Asking questions in a way which does not make the interviewee feel intimidated or uncomfortable;
- Conducting the interview in familiar surroundings as this will be less intimidating;
- Encouraging co-operation by allowing witnesses to speak openly in their own words without using technical jargon;
- Promoting a positive attitude to finding the reasons for the incident to prevent a recurrence in the future rather than apportioning blame for the present one;
- Interviewing witnesses separately and in private to prevent them from influencing each other’s accounts;
- Providing a summary of what the witness said in order that they can ensure that everything has been understood correctly and that the interviewer has not misinterpreted the account.
Gathering the information – plans
After the incident, any plans or sketches of where people were at the time as well as the layout of the area (e.g. machinery) will be helpful in finding the causes of the accident/incident.

Gathering the information – photographs
Photographs can provide evidence of the scenes of an incident immediately after the event. This is important because investigations can be ongoing and evidence may be lost.
Gathering the information – relevant records and sources of information
The amount of information and evidence required after an incident depends upon the seriousness of the outcome. They may include the following:
- Victim statements;
- Witness statements;
- Plans and diagrams;
- CCTV coverage;
- Process drawings, sketches, measurements, photographs;
- Check sheets, permits-to-work records, method statements;
- Details of the environmental conditions at the time;
- Written instructions, procedures and risk assessments which should have been in operation and followed;
- Previous accident records;
- Information from health and safety meetings;
- Technical information/guidance/toolbox talk sheets;
- Manufacturers’ instructions;
- Risk assessments;
- Training records;
- Logs;
- Instrument readouts and records;
- Opinions, experiences, observations.
The accident/incident investigation step 2 – analysing the information
Any analysis of the information collected should:
- Be objective and unbiased;
- Identify the sequence of events and conditions that led up to the event;
- Identify the immediate causes;
- Identify underlying causes, i.e. actions in the past that have allowed or caused undetected unsafe conditions/practices;
- Identify root causes, i.e. organizational and management health and safety arrangements – supervision, monitoring, training, resources allocated to health and safety, etc.
Analysis of this information should result in supplying reasons why the incident happened. It may also become clear what further information is still required. It is useful to analyse information gathered as an ongoing process during the investigation, as this will allow for other lines of enquiry to evolve and be developed.
By involving all members of the investigative team, differing opinions can be considered and a broad view of the results gained. The analysis should be conducted systematically to make sure nothing has been missed and that an unbiased outcome can be reached as to the immediate, underlying and root causes of the accident. We shall be looking at these types of causes in more detail later in this chapter.
The accident/incident investigation step 3 – identifying the required risk control measures
Once the findings of the investigation have evolved, they will highlight failings in the existing control measures which led to the incident. They may also determine which control measures should be implemented in order to prevent a future recurrence. Another outcome of an accident investigation is that it will prioritize the risk control measures to be implemented.
Usually those control measures which eliminate the risk by using engineering controls are more reliable than those controls which are reliant on people.
There is a ‘hierarchy of risk control’ which should be put in place in the following order:
Hierarchy of risk control
- Eliminate the risk altogether;
- Substitute the risk for something safer;
- Apply engineering controls such as cut out devices, guards, etc;
- Apply administrative controls such as safe working practices;
- Use Personal Protective Equipment (PPE), but only as a last resort or in conjunction with other controls.
The accident/incident investigation step 4 – formulation of the action plan and its implementation
The involvement of senior management in the formulation of an action plan will be necessary, as this level of management is generally the decision-making level within an organization. The investigation team will recommend additional risk control measures which have been determined as a result of the investigation. The action plan will determine which control measures should be implemented in the short term and others which will be long term measures.
The action plan should have SMART objectives, i.e. be:
- Specific;
- Measurable;
- Achievable;
- Realistic, and with;
- Timescales.
The accident/incident investigation – analysing the causes
We will now take a more detailed look at the process of analysing the cause of an incident. Causes of incidents can be categorized into three basic types – immediate causes, underlying causes and root causes.
- Immediate causes are generally unsafe acts and/or conditions;
- Underlying causes are generally procedural failures;
- Root causes are generally management system failures.
Immediate cause
The most obvious reason why an adverse event happens, e.g. the guard is missing; the employee slips; the pipe flange fails,etc. There may be several immediate causes identified in any one adverse event.
Immediate causes are those which are responsible for the accident and are often easy to recognize.
Underlying cause
The less obvious “system” or “organizational” reason for an adverse event happening, e.g. pre-start-up machinery checks are not carried out; safe working procedures are not adhered to; the hazard has not been adequately considered via a suitable and sufficient risk assessment; production process pressures are too great, etc.
Root cause
Root causes are generally management, planning or organizational failings. For example, we mentioned safe working procedures not being adhered to, as an underlying cause. This could be because of lack of training or poor supervision, both of which are classed as root causes. Other examples of root causes include:
- A lack of rules and/or working procedures;
- Insufficient training;
- A general lack of commitment to safety;
- Insufficient supervision;
- Poor plant, equipment and layout design;
- Poor working conditions.
Analysing causes of an accident
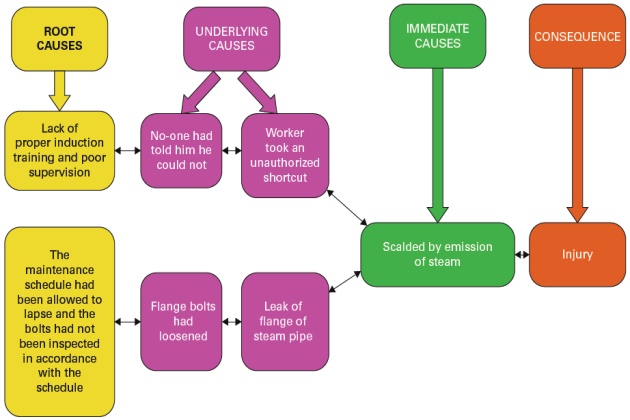
There are many techniques used in determining the true picture of immediate and root causes of an accident/ incident, one of which is by applying a questioning technique which constantly asks “why?”, and then applying the answers to a pictorial diagram which gives a causal tree analysis. If we apply this technique to the accident outlined below we can see how it works.
We start by looking at the ultimate consequence and work our way back by asking “why?”. We can then get a full picture of all the causes.
Let’s ask the questions “why?” to our situation and see what transpires.
Joe is one of the control room operators on board a floating production storage and offloading (FPSO) platform.
He had been asked to inspect a fire and gas sensor some distance away from his normal work post. He decided to take a shortcut through an area that housed steam pipes.

Unauthorized employees are not normally allowed in this area as the steam in the pipes is under pressure and of high temperature. As he was passing by the piping, one of the flanges of the steam pipes emitted a blast of steam which scalded Joe’s hand and he suffered serious burns.

Joe was a walking wounded casualty and took himself to the medical bay for treatment to burns. An investigation into the incident was started.
Let’s now work our way through the investigation of the accident involving Joe by asking a series of questions. These questions are meant to unfold the facts as they reveal themselves, much like the layers of an onion.
We start with the known fact that “a person has been injured in an area housing steam pipes”. From there we keep asking the question “why?” in order to reveal the underlying cause(s) of each element as it is revealed. Let’s have a look at how it works.
Fact – A person (Joe) has been injured in the area housing steam pipes.
From this investigation, we can now build up a causal tree showing:
- Immediate causes;
- Underlying causes;
- Root causes.
As you can see, the causal tree we have been able to draw from constantly asking the question “why?” has given us a clear picture of what all the true causes of the accident were.
This leaves us with a clear indication of the actions which need to be taken if we want to ensure there is no repetition of any of the events leading up to the accident.
Accident/incident report forms
There are many kinds of accident/incident report forms but all do the same job – they all include the findings of the investigation and determine the causes of the incident. They also provide recommendations to prevent further occurrences. There are also various computer programs which have been developed to record and analyse data. Whatever the format, they all state:
- What happened – the injuries/losses/costs;
- How it happened – the event itself;
- Why it happened – the causes: root, underlying and immediate;
- Recommendations – any action to be taken to remedy the situation and prevent any recurrences.
The use of standardized report forms ensures that the investigation process is correctly adhered to and that information can be reported back to management. Follow-up actions can easily be taken following appropriate recommendations within the report. Standardized report forms can also act as a checklist.
An efficient recording system will:
- Ensure the information is correctly and accurately presented;
- Allow the data to be analysed easily in order to discover common causes or trends;
- Ensure data which may be required for future reference is included;
- Identify issues which may help prevent any recurrence of the accident.
Report forms should be reviewed on a regular basis to ensure that any recommendations have been implemented.
The importance of learning lessons from major incidents, management, cultural and technical failures that may lead to such incidents
Learning the lessons
The lessons learned from accidents and incidents all contribute to the building up of knowledge and experience which can help in avoiding a repetition of such events. This is because the consequences of accidents in the oil and gas industry can be catastrophic, e.g. Deepwater Horizon, Piper Alpha, Buncefield, etc. Acquiring knowledge and experience from accidents and incidents should be a structured process, whether it is a minor accident or a major incident. It is important that lessons learned stem from a basic understanding of the incident in order to develop a safety culture which can be vital in avoiding a major catastrophe.
Learning lessons from an incident can benefit two main areas:
- Locally – the people directly involved, in order to prevent a recurrence of the incident;
- More widely – to ensure that the experience and lessons learned from one incident involving one system can be shared with other systems, thus avoiding similar incidents in other areas.
Learning lessons locally
At the end of the investigation there needs to be a dissemination of the conclusions arrived at from all of the information which has been collected and analysed. It is important that these are communicated in a way that is understood by everyone, in a format which is appropriate to the level necessary. For example:
- For the management of the organization – they will need a report which details:
- what went wrong;
- the systems and procedure failures which were involved;
- how serious the incident could have been;
- how to avoid future incidents.
- For regulatory bodies, safety records, etc. – technical details of the investigation as well as its findings;
- For operators of the systems and procedures involved in the incident – the findings and recommendations of the investigation should be in a format which is understandable at their level. This will allow changes to be made in order to prevent future incidents. The format could be in the form of checklists, written procedures, etc;
- For incident investigators generally. This group of people have an ongoing need to broaden their knowledge and understanding of how things go wrong and how to encompass this knowledge in future investigations.
Training and educational materials should also be in an appropriate format tailored to the target audience. These could be in:
- A written format – guidance notes, checklists, written procedures. If checklists are used it is important that they are not used in isolation but alongside other materials which give explanations of each item listed in order to make full use of the background knowledge and experience gained from an investigation;
- Audio-visual aids to convey the information – these can be training videos, which for some people are preferable to other methods of teaching;
- Verbal presentations – face-to-face teaching sessions which include explanation of the investigation
and its findings from both the perspective of the investigator(s) and those who were involved in the accident; - Training exercises – these could be simulations of incidents which would include exercises on how to deal with actual events should they occur, or even scenarios based on previous incidents using the personal accounts of those involved.
To promote a culture of learning within an organization, it is important that any lessons learned, and experience gained, are used effectively when new projects are planned or existing ones modified. The experience of others can be used in such techniques as “peer assist”. Peer assist is a technique whereby a group of people who have been involved in investigating incidents can share their experiences and lessons learned with others who may have to conduct investigations in the future.
Learning lessons more widely
Lessons learned within one organization can be disseminated widely throughout other organizations by the publication of information in trade or specialized journals or publications, or through internet websites. People who prepare information to be disseminated need to make it interesting and well presented. The author should be able to:
- Highlight relevant points which are of interest to the target audience;
- If using first-hand accounts, be concise so that the information has maximum impact;
- Use examples of different incidents to illustrate similarities and differences, but avoid repetition in order to maintain interest in the article;
- At the end of the article, summarize the information and provide a conclusion;
- Supplement the article with trend information People who have first-hand knowledge and experience of an incident and dealing with the aftermath can be instrumental in teaching others. They can be involved in running workshops and providing presentations or training sessions.
As well as individuals disseminating knowledge and experience internally within their companies, there should be systems in place whereby these people can share their experience and knowledge with other organizations and agencies in order to broaden the range of beneficiaries. This could take the form of trade activities or training sessions where representatives of companies attend and where incidents are discussed. The information can then be reported back to be shared within their own companies.
The contra position of learning lessons is where lessons are simply ignored or abandoned, and in these cases the consequences can be catastrophic.
In the Piper Alpha case, the positioning of dangerous operations away from personnel areas had been recognized as a move towards a safer operating environment. However, when gas production began on Piper Alpha, a propane condensate pump was positioned near the control room for pure convenience. This disregard for lessons learned proved to be a fatal error in the consequences that followed.
It is a part of safety requirements in the oil and gas industry that companies take into consideration safety information, not only from within their own organization, but from other organizations, when assessing risks.
Revision questions for element 1
Answer 1
There are two main reasons why an accident/incident should be investigated. The first reason is to determine the cause of the accident/incident. The second reason is to use the information forthcoming from the investigation to take corrective action in order to avoid it happening again.
Answer 2
- Step 1 – Gather the information.
- Step 2 – Analyse the information.
- Step 3 – Identify the required risk control measures that will reduce the risk.
- Step 4 – Formulate an action plan and implement it.
Answer 3
- Victim statements.
- Witness statements.
- Plans and diagrams.
- CCTV coverage.
- Process drawings, sketches, measurements, photographs.
- Check sheets, permit-to-work records, method
statements. - Details of the environmental conditions at the time.
- Written instructions, procedures and risk assessments which should have been in operation and followed.
- Previous accident records.
- Information from health and safety meetings
- Technical information/guidance/toolbox talk sheets.
- Manufacturer’s instructions.
- Risk assessments.
- Training records.
- Logs.
Answer 4
A near miss is any unplanned incident, accident or emergency which did not result in an injury but which could have done in slightly different circumstances.
Answer 5
A near miss should be investigated because any recurrence may result in a more serious outcome. Consequently, an investigation should be conducted to determine its cause so that changes can be made to prevent it happening again.